Heart disease exposes disparities, so medicine goes mobile in Detroit

DETROIT — Death comes early to Detroit, killing residents in some neighborhoods 12 to 15 years earlier than Michiganders elsewhere.
Thickening heart muscles, narrowing arteries and cholesterol deposits are hallmarks of the heart disease silently afflicting Detroiters and building toward life-threatening heart attacks or strokes.
Health Care for Some
This is one in a series of reports focusing on health disparities in Michigan. The project was made possible by a grant from the nonpartisan, Washington-based National Institute for Health Care Management (NIHCM) Foundation. If you have suggestions for future coverage please contact Robin Erb at rerb@bridgemi.com
Patients arrive at Detroit’s Sinai-Grace and Receiving hospitals with blood pressure “through the roof,” sometimes double the normal range, said Dr. Brian O’Neil, chair of emergency medicine at Wayne State University’s School of Medicine. Young doctors arriving in Detroit to train, he said recently, are often “blown away” by the readings.
Related:
- 2020: Black communities hit harder by coronavirus in Michigan, not just Detroit
- 2020: As coronavirus bears down, Detroit enters a grim new phase
Days earlier, emergency crews brought in a 47-year-old man they believed overdosed on drugs, O’Neil recalled. In reality, the man was suffering from an irreversible brain bleed caused by a hypertensive crisis. His blood pressure, at 237/128, was well above normal, O’Neil said, and he will likely end up in a nursing home with “astronomical” health care bills.
COVID-19 made it worse
The coronavirus has layered exorbitant deaths and collateral stress, especially among communities of color, upon the generations of heart disease and other chronic conditions Detroiters face. It has exacerbated chronic conditions and increased the number of deaths of preventable diseases because people, fearing contracting the virus, skipped regular check-ups, hesitated to call 911 when they faced symptoms of illness and steered clear of the emergency room.
In 2020, the virus also disrupted transportation in Detroit, making it more difficult for some to get to doctor’s appointments or be with loved ones who could intercede in an emergency
The result: More people who suffered heart attacks or strokes died because they lacked swift medical intervention.
The rate of heart-related deaths inched 3 percent upward — to 167 deaths for every 100,000 residents in 2020 from 162 deaths per 100,000 in 2019. In Detroit, age-adjusted heart disease-related deaths surged nearly 18 percent — to about 340 for every 100,000 residents in 2020 from about 289 deaths per 100,000 residents in 2019.
But the pandemic did something else too: It proved the nimble nature of mobile health to follow disparity data and address the issues.
Narrowing in on the problem
Dr. Phil Levy, an emergency medicine doctor at Detroit’s Receiving Hospital and Wayne State University researcher, was perfectly positioned to act.
His weapon: Piles of data that he and his team gathered and arranged in color-coded maps.
For several years, Levy and his research team worked on a data tool, called Population Health OutcomEs aNd Information EXchange, or PHOENIX — that mapped out hypertension rates in the Detroit area by superimposing layers of data onto the city map and its surrounding regions. They collected more than a half-million “encounters,” or emergency room visits, arrivals driven not only by heart attacks, strokes and other crises related to high blood pressure, but also by concerns like earaches and broken bones.
Afterward, they stripped personal identifiers from the readings, assigning the data to census tracts where patients lived. They then added more data to the tracts, including patient age, employment and graduation rates in the neighborhood, poverty estimates, crowding metrics, disability rates, and other measures that help rank neighborhoods based on socioeconomic status.
The result was a Detroit sliced into census tracts and color-coded to reveal “hypertension hot spots” or neighborhoods strained by high blood pressure and stress based on social vulnerability index factors.
The process allowed Levy to get a clearer sense of the larger reality:
Heart disease has been killing Michiganders at a far greater clip than most other Americans for at least 20 years, according to the Michigan Death Certificate Registry. Just six states had higher rates of heart disease in 2020 than Michigan, according to data from the U.S. Centers for Disease Control and Prevention.
The toll is more staggering in Detroit — where heart disease consistently kills residents about 1.6 times more often than others, according to state data.
Because heart disease is the nation’s leading cause of death, the resulting disparities in life expectancy are stark.
About half of city residents in more than two dozen metro Detroit census tracts will die before their 70th birthday, according to the mapping system researchers at Wayne State created. In comparison, life expectancy for about half of U.S. residents in 2018 was more than 78 years.
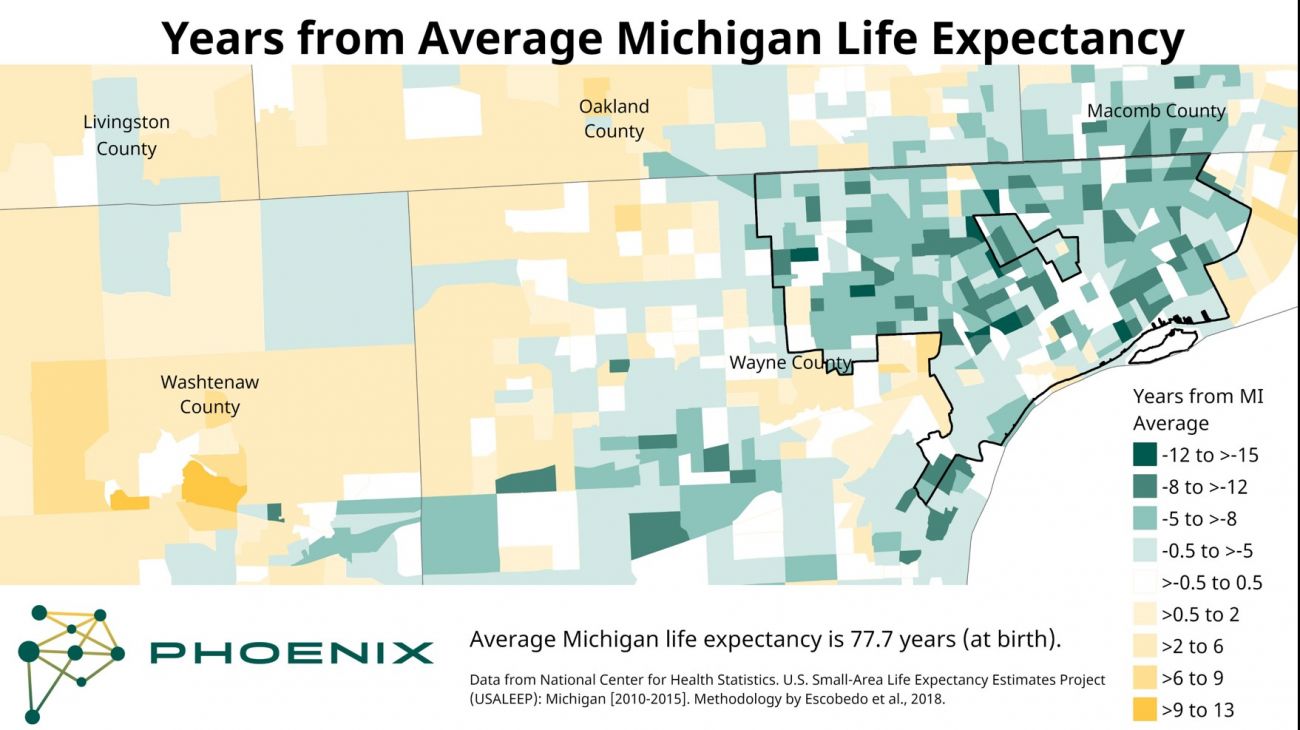
Just a few miles away, Macomb, Oakland and Washtenaw county residents in many neighborhoods can expect to live into their 80s.
Levy’s ultimate research goal was to find ways to reach into underserved communities and help people control hypertension before it spiraled out of control. However, when COVID slammed into Detroit in the spring of 2020, Levy set his data project aside.
Yet even in the earliest days of the pandemic, the parallels between COVID and heart disease in Detroit were obvious, he said.
“We started seeing everything that was happening with the brown and Black communities in Detroit and around Detroit — especially around the Sinai Grace area — and the increased caseload and death rate that was occurring in Detroit,” Levy said.
As more patients in their 40s and 50s suffering from cardiac crises began arriving with lights and sirens, “we started to really ask ‘What the heck is going on here?”
It was evident early on that Black residents were dying from COVID at a much higher rate than their white counterparts. According to the Michigan Department of Health and Human Services, Black Michiganders — which make up just 14 percent of the state’s population — represented 40 percent of the COVID deaths in the first month of the pandemic.
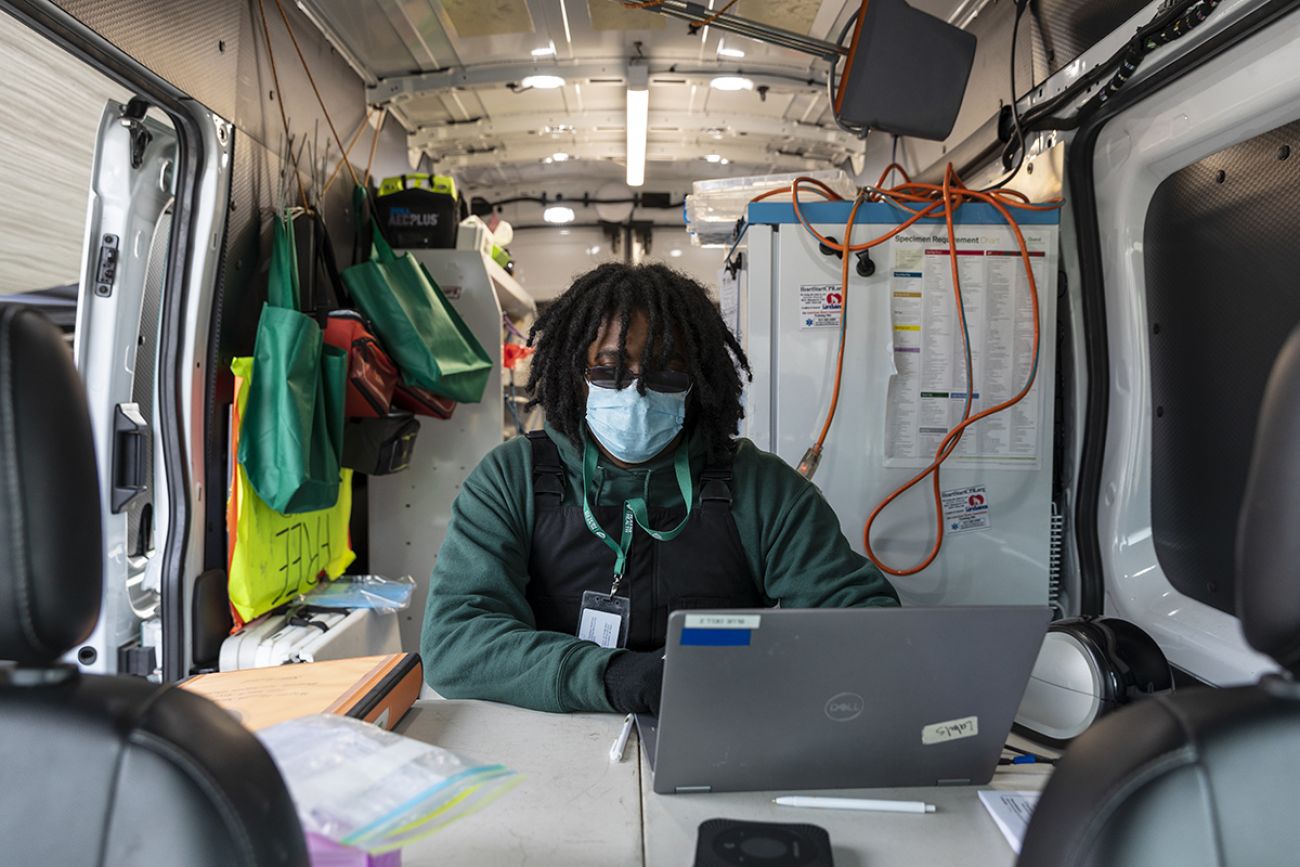
In April, as the country was struggling to get mass testing programs up and running, Levy and his team loaded up a new Ford Transit van to help test and clear first responders for duty.
Levy also turned back to his PHOENIX software mapping tool and superimposed more layers of data, including positive COVID test results.
As it did with hypertension rates in the city, the map spotlighted areas most hammered by the new virus.
The data was clear, he said. “The vast majority of people dying from COVID [come] from socially vulnerable communities with a high degree of comorbidities — meaning hypertension, diabetes, heart disease and kidney disease.”

Detroiter James Young, an American Heart Association volunteer, said COVID also fueled social drivers of health inequities, including generations of distrust of the health care system that historically mistreated Black Americans — as they did with the infamous Tuskegee experiment.
As a result, less than half of Black Americans wanted to receive COVID vaccines compared to 61 percent of whites, according to a November 2020 Pew Research Center survey.
Some worried, too, about medical bills, Young said.
In 2011, those worries put Young, then a 40-year-old part-time web manager making less than $40,000 a year, in danger. He earned too much for free health coverage but not enough to afford the monthly premiums, he said.
Then he got sick.
“I’d gone days and days without sleeping,” he said, “and just didn't have the energy to do anything.”
In the waiting room at Covenant Primary Care in Royal Oak, he grew increasingly restless and jittery.

He stepped outside. He thought the sky was beautiful. Then he noticed his chest rising and falling with surprising force. “Strange,” he thought, because the concomitant air didn’t seem to come.
What followed was a slow-motion commotion. A knot of people. “Emergency room, now!” someone said.
“I was a walking heart attack or a walking stroke,” said Young. Since September 2011, he has lost 100 pounds, mostly in the fluid that his heart had been too overwhelmed to pump.
The diagnoses — congestive heart failure, cardiomyopathy and chronic kidney disease — shocked him.
“The biggest problem with hypertension is you don't feel bad until you feel really bad,” said O’Neil, an emergency room doctor. “High blood pressure doesn't give you a ton of symptoms until you have a bleed in your brain, or you have a heart attack, or you've ruined your kidneys.”
Behind the wheel
As COVID wore on in 2020, Levy’s team rerouted the transit van, loaded with testing supplies and later vaccines, into Detroit neighborhoods, many of which housed older residents who are more vulnerable to COVID.
Levy’s van reached 32,523 people through 491 testing and 19 vaccination events in one year, according to a report the doctor published in the peer-reviewed journal PLoS One. The program grew to five mobile units that year.
The teams expanded into lipid testing and blood pressure measurement, lead testing and needle exchange programs, mental health and substance abuse disorder screening.
As the mercury hovered just above freezing in January this year, several of Levy’s staff, armed with nasal swabs and vaccines, ran between a mobile health unit and a line of vehicles and then warmed themselves by a portable gas heater.
“If we can get [residents] to stick around long enough, we can take their vital signs, height and weight. We put a pulse ox on them, and a blood pressure cuff,” said Alexander Molex, 22, the mobile health unit site leader that day.
If the blood pressure is too high, staff can set up a follow-up appointment with a primary care physician and connect them to programs for free medication and even transportation, he said. Many of the encounters, he said, are with residents who otherwise wouldn’t see a doctor.
Often, they’re not poor.
“Whenever we think of health disparities, we always think of the uninsured and those who are impoverished, but they’re not the only ones affected,” Levy said.
“You have a lot of people who are working in the manufacturing ecosystem, for instance, on an assembly line who are hourly employees. They may get health insurance or may not through their work, but they can't leave work to go do a routine physical.”
At the Wright Museum's 39th African World Festival in downtown Detroit earlier this summer, 20-year-old Wayne State University student Soneet Kapadia helped staff a health van.
The evening was festival-perfect — the smell of grilled food drifting along the sidewalks and music pumped by speakers into the early-evening air. Passersby carried oversized pineapple drinks.
“We go where we can reach people. We hit the problem at the source,” Kapadia said.
Nearby, Jose Gomez was collecting blood from Leslie Huffman, 64, a stage manager who was helping to set up the night’s music offerings.
She hadn’t been thinking about her health, but she plopped down in a folding chair and cracked jokes with staff as they drew her blood for a series of tests.
“They’re here. I’m here. Easy,” she said.
No quick answers.
In his office on Mack Avenue, Levy flipped through color-coded maps and bar graphs of data that can help lead to a healthier city and individuals who will enjoy longer, more active lives.He’s sure of it.
It will take years to see if he’s right.
“It’ll be 40 years, but it's a long game, right?” Levy said. “If I'm looking at the success as measured by ‘Did I get this one person's blood pressure under control?’ That's the wrong metric. The metric is ‘Did I get this community healthier, and do people live longer?’ That’s ultimately why it matters.”
Levy’s team now has more than 70 paid employees, including medical assistants, patient service representatives, community health workers, nurses and nurse practitioners. And his program receives funding from the National Institutes of Health, the Michigan Department of Health and Human Services and nonprofits such as o the W.K. Kellogg Foundation, the Ralph Wilson Foundation, the United Way for Southeastern Michigan (which also are funders of the Center for Michigan, Bridge Michigan’s parent company), the Community Organized Relief Effort, BCBS of MI Foundation and Bank of America.
In all, a whopping $41 million of funding has flowed into Levy’s effort, nearly all of it since the first van hit the streets of Detroit to do mobile testing, and later to administer vaccines.
Is it worth it?
Consider the costs of uncontrolled hypertension, which leads to heart disease, stroke and kidney failure, as well as higher health-care costs, long-term care and lost work time, said Dr. Pino Colone, an ER doctor at Henry Ford Health and the immediate past president of the Michigan State Medical Society
The problem of health disparities can be overwhelming; mobile health efforts can chip away at them, he said.
“We really can't afford not to try these things,” he said.



See what new members are saying about why they donated to Bridge Michigan:
- “In order for this information to be accurate and unbiased it must be underwritten by its readers, not by special interests.” - Larry S.
- “Not many other media sources report on the topics Bridge does.” - Susan B.
- “Your journalism is outstanding and rare these days.” - Mark S.
If you want to ensure the future of nonpartisan, nonprofit Michigan journalism, please become a member today. You, too, will be asked why you donated and maybe we'll feature your quote next time!